
Do Antidepressants Work? A People’s Review of the Evidence
Do Antidepressants Work? A People’s Review of the Evidence


In late February, newspapers in the UK and elsewhere announced that a new meta-analysis published in Lancet had proven, once and for all, that “antidepressants work.” The lead author of the paper, Andrea Cipriani, and other psychiatrists from the Royal College of Psychiatry in the UK, declared that this was a definitive study, and that any debate over the drugs was now over. This led at least a few newspapers to dust off their Prozac headlines from 25 years ago and declare that “Happy Pills” were here again.
Joanna Moncrieff and others have written detailed critiques of that study. Their most important point is that this meta-analysis relied on an outcome measure that inflates the perceived efficacy of the drug. Otherwise, the study provided little that was new. Previous meta-analyses of the literature for antidepressants had found that their effect size was small to moderate over the short term, with these results mostly coming from industry-funded trials, and the Cipriani study, when carefully parsed, found the same thing.
Unfortunately, it is the “antidepressants work” soundbite that will remain in the public mind and not the critique. And here’s the problem: there is a need for the public to know the many types of evidence that bear on this question of whether antidepressants “work.” Psychiatry relies on a particular slice of evidence — RCTs in a carefully selected group of patients — to support its “antidepressants work” message. But a review of the evidence regarding their effectiveness
Personally, I think the question — do antidepressants work — is a poor way to frame this debate. Some people respond well to antidepressants, some do so-so on the drugs, and others worsen. Furthermore, this spectrum of outcomes occurs in comparison to natural recovery rates, which also need to be fleshed out. Thus, the challenge is to review the evidence in a way that best illuminates the risk-versus-benefit equation for individual patients. That is what is necessary for informed consent, which is fundamental to the practice of ethical medicine.
There are three parts to the review that follows:
- The evidence for the efficacy of antidepressants over the short term in RCTs, which is the evidence that psychiatry relies on to claim that the drugs “work.”
- The evidence for the effectiveness of antidepressants over the short term in “real-world” patients.
- The evidence regarding their long-term effectiveness in real-world patients.
This broader review of the research literature does then lead to a dichotomous question for society. Do antidepressants, as they are being prescribed now, “work” for society? Do they produce a public health benefit?
Efficacy of antidepressants in RCTs
As Moncrieff noted in her critique, meta-analyses of RCTs assessing the short-term efficacy of antidepressants may give a skewed view of the drugs, simply because the RCTs are fraught with problems. Most of the studies are industry-funded; investigator bias is a worry; the placebo group is composed of patients who have been abruptly withdrawn from their drugs, which isn’t a true placebo group at all; negative results go unpublished; and the studies are conducted in a small subset of patients who could be expected to best respond to a drug. All of these shortcomings with the RCT literature bias outcomes in favor of the antidepressants.
Even so, the evidence of antidepressant efficacy that emerges from RCTs is, at best, a modest sort.
Symptom reduction scores
Irving Kirsch and his collaborators, in their meta-analyses of industry-funded RCTs, have reported that the difference in symptom reduction between the medicated and placebo groups is less than two points on the Hamilton Rating Scale of Depression (HAM-D). The National Institute of Clinical Excellence in the UK has stated that there needs to be at least a 3-point difference on this scale to be clinically relevant, and Kirsch found that it was only in a subset of patients, those severely depressed, that SSRIs met this standard.
Kirsch and others have calculated “effect sizes” of around .30 for antidepressants based on symptom scores. As is shown by the graph below, this means that there is an 88% overlap in the distribution of outcomes for the drug-treated and placebo patients.

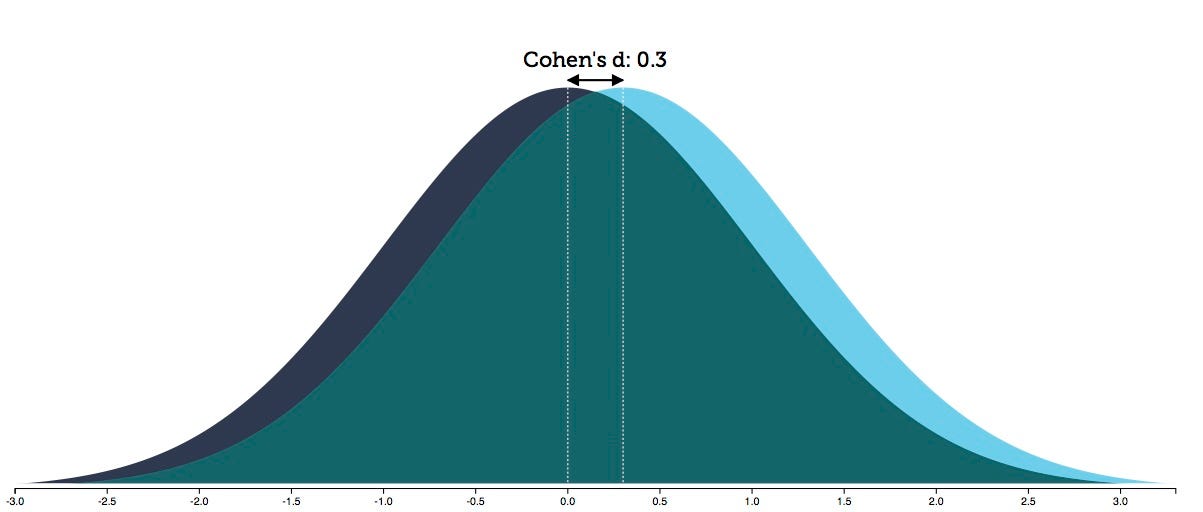
Given the placebo response rate in these trials, an effect size of .30 produces an NNT — number needed to treat — of 8. This means you need to treat 8 people to produce one additional person who benefits from the treatment, as compared to placebo.
Thus, the risk benefit equation from this symptom-reduction data can be summed up in this manner: Is exposure to the adverse effects of drug treatment worth the 12% chance of a better outcome? Or to put it another way: 12% of patients will benefit from the treatment, while the remaining 88% will suffer the adverse effects of treatment without any additional therapeutic benefit beyond placebo. Those are the odds that a person contemplating taking an antidepressant drug might want to know.
Response rates (at eight weeks)
In their Lancet study, Cipriani and colleagues relied on “response rates” to assess the efficacy of antidepressants. Response was defined as a 50% reduction in symptoms. The researchers then calculated the “odds ratios” for the response rates in the two groups, which tells of a relative efficacy. How much more likely is it that patients in one group will be responders compared to patients in the second group? Cipriani reported that the “odds ratios” favored the antidepressant over placebo in every case, with the “ORs” ranging from 1.37 for the least effective antidepressant, and 2.13 for the most effective one.
Kirsch and Moncrieff, as well as others, have noted that using response rates as a measurement inflates the perceived efficacy of the drug, and it is easy to understand why. A patient who has a 52% reduction in symptoms on the HAM-D will be classified as a responder, while a patient who has a 48% reduction in symptoms will be classified as a non-responder, even though there is no real difference in improvement between the two. As a result, a slight difference in HAM-D scores between drug and placebo groups may show up as notably increasing the likelihood that a person will “respond” to the drug treatment.
Unfortunately, Cipriani and colleagues didn’t report the response rates that were used to calculate the odds ratios, which is the very information that the public would like to know. Do 25% of people “respond” to antidepressants? Fifty percent? Seventy-five percent? There is no way to answer such questions from the odds ratios alone. Thus, the very study being touted as proving that “antidepressants work” fails to give any information about what percentage of people “respond” to the medication.
However, other meta-analyses of RCTs of antidepressants have reported mean placebo response rates of around 37% for the placebo group and 60% for the antidepressant group, which fits with the overall odds ratios published by Cipriani. In terms of the risks and benefits of taking an antidepressant, this outcome can be interpreted in this way:
- Thirty-seven percent of patients would respond without treatment, and thus treatment exposes them to the adverse effects of antidepressants without any additional benefit. As such, they could be said, on balance, to have been harmed by the treatment.
- Forty percent of patients will be non-responders to the treatment, and yet will be exposed to the adverse effects of antidepressants. They too could be said, on balance, to have been harmed by the treatment.
- Twenty-three percent of patients will be responders to the treatment who otherwise would be non-responders. This is the group that could be said to have been helped by the treatment.
In sum, in terms of assessing risks versus benefits based on response rates, 77% of all patients will be exposed to the adverse effects of the drug while receiving no extra therapeutic benefit. Only 23% will experience a therapeutic “response” that they otherwise wouldn’t have had. This produces an NNT of 4, and while this is twice as good as the NNT calculation based on the symptom scores, it still leaves three out of four patients experiencing the adverse effects of antidepressants without any benefit beyond placebo.
Both of these methods of assessing efficacy in RCTs — symptom reduction and response rates — provide evidence that, in statistical terms, “antidepressants work.” But it is easy to see that in terms of evaluating the risks-versus-benefits for the individual patient, they provide no such certainty.
Short-term effectiveness in “real-world” patients
As Cipriani and colleagues noted, industry-funded RCTS are conducted in a select set of depressed patients — those without comorbidities or suicidal thoughts. In essence, the pharmaceutical companies use eligibility criteria to select a group most likely to respond well to the drug. Only about 10% to 30% of real-world depressed patients meet these criteria.
With this thought in mind, John Rush, a prominent psychiatrist at the University of Texas Southwestern, conducted a study in 2004 of the effectiveness of antidepressants in 118 real-world patients. Effectiveness describes outcomes in real-world settings, as opposed to the drug “efficacy” that is measured in RCTs, and thus this is the outcome data that would be most relevant to patients.
The patients in Rush’s study, who were seen in an outpatient setting, were given the best clinical care possible. Yet only 19% had responded to the treatment at three months, which was one-third the response rate recorded in RCTs.
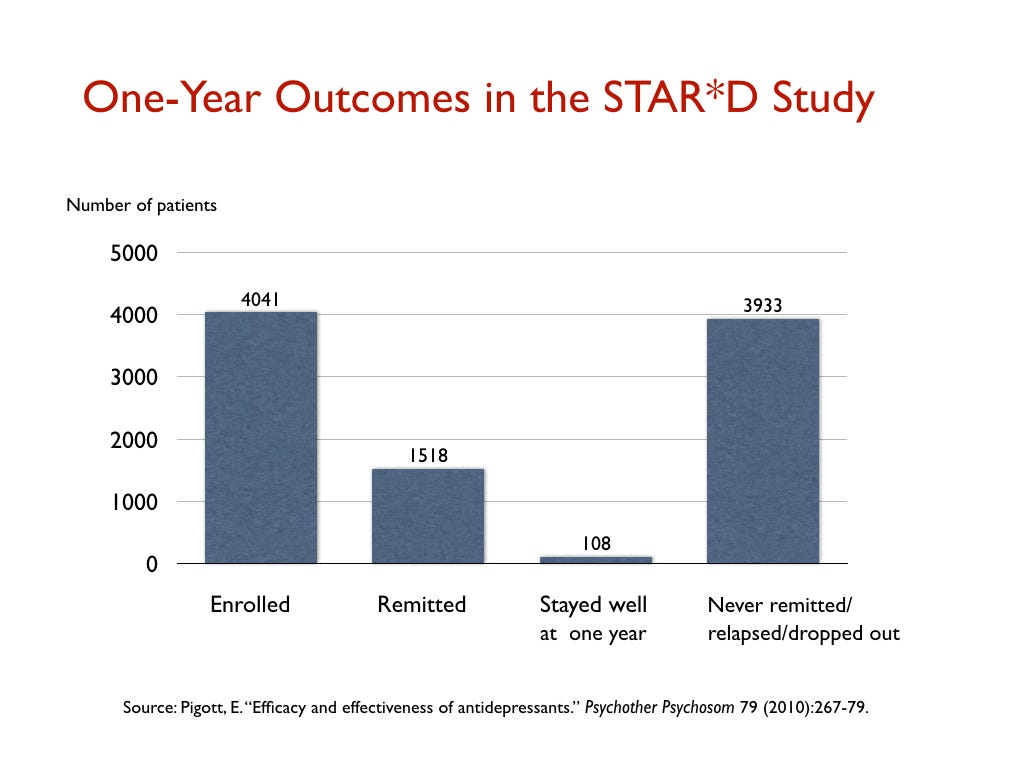
Rush was also a lead investigator in the NIMH’s STAR*D study. This was hailed as the largest antidepressant study ever, and it too was meant to assess the effectiveness of antidepressants in real-world patients, most of whom were only mildly to moderately ill. Moreover, the study had a design that could be expected to produce a higher response rate than usual in an RCT. Patients who didn’t respond to a first round of treatment could then have a second round with a different antidepressant, and so on through four courses of treatment. The idea was that eventually a treatment would be found that would work, with patients given multiple chances to register a HAM-D score of seven or below. Yet, even with this design, only 38% of the 4041 patients reached this level of improvement.
These real-world response rates reported by Rush raise an obvious question: Are they better than “natural recovery” rates over the short term? I am not sure there is a good answer to that question in the research literature, but what can be concluded from these two studies is that there is a lack of evidence that antidepressants are effective in the majority of real-world patients, even over the short term. They “work” in only a minority of patients, and it may be that they don’t provide any benefit over natural recovery rates at the end of 6 to 12 weeks.
Long-term effectiveness in real-world patients
Remission rates
The goal for people who are depressed is to get well and stay well. In research terms, patients want to experience a “sustained remission.”
In Rush’s study of 118 real-world patients, 13% were in remission at the end of the year, but only 5% had a “sustained remission” during the year. The outcomes in his study, Rush confessed, “reveal remarkably low response and remission rates.”
The documented stay-well rate in the STAR*D trial was even worse. At the end of one year, only 108 of the 4041 patients (3%) had remitted and stayed well and in the trial. All of the others had either failed to remit, relapsed, or dropped out of the study.

A Minnesota report on the real-world outcomes of 260,000 patients treated for depression from 2010 to 2013 found similarly low remission rates. At the end of each year, only about 5% of the patients were in remission. Another 10 percent or so were still considered responders to antidepressant treatment. The remaining 85% were categorized as chronically depressed.


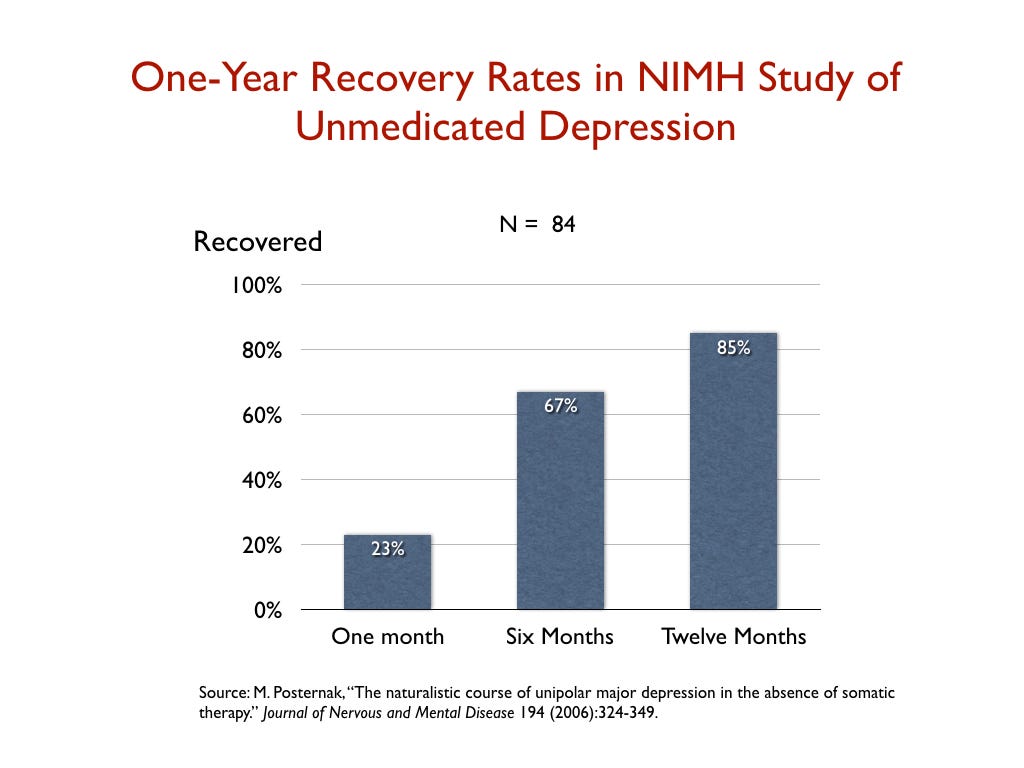
In 2006, Michael Posternak, a psychiatrist at Brown University, studied the one-year remission rate for unmedicated patients. To do his research, he identified 84 patients enrolled in an NIMH study who, after recovering from an initial bout of depression, subsequently relapsed but then did not go back on an antidepressant. He tracked their remission rate over time: 23% percent had recovered by the end of the first month; 67 percent at the end of six months; and 85% at the end of one year.
Posternak summed up his results in this way: “If as many as 85% of depressed individuals who go without somatic treatment spontaneously recover within one year, it would be extremely difficult for any intervention to demonstrate a superior result to this.”

Now it is possible that these various “effectiveness” studies, for one reason or another, assessed recovery rates in patient cohorts that were quite different. Even so, it is notable that the one-year outcomes for the medicated and unmedicated groups in these studies were the polar opposite of each other: 85% of the medicated patients were chronically depressed, while 85% of the unmedicated patients were in remission. As the graphic below shows, this comparison demands further investigation.


Naturalistic studies of unmedicated v. medicated depression
There have been a handful of naturalistic studies during the SSRI era that have compared longer term outcomes for patients who chose to take antidepressants and those who did not, with these studies helping to flesh out the evidence regarding the “effectiveness” of these drugs in real-world patients. Specifically:
- In a 1997 study of outpatients at a large inner-city clinic in the UK, 95 never-treated patients saw their symptoms decrease by 62 percent in six months, whereas the 53 medicated patients experienced only a 33 percent reduction in symptoms. The medicated patients “continued to have depressive symptoms throughout the six months,” the investigators reported.
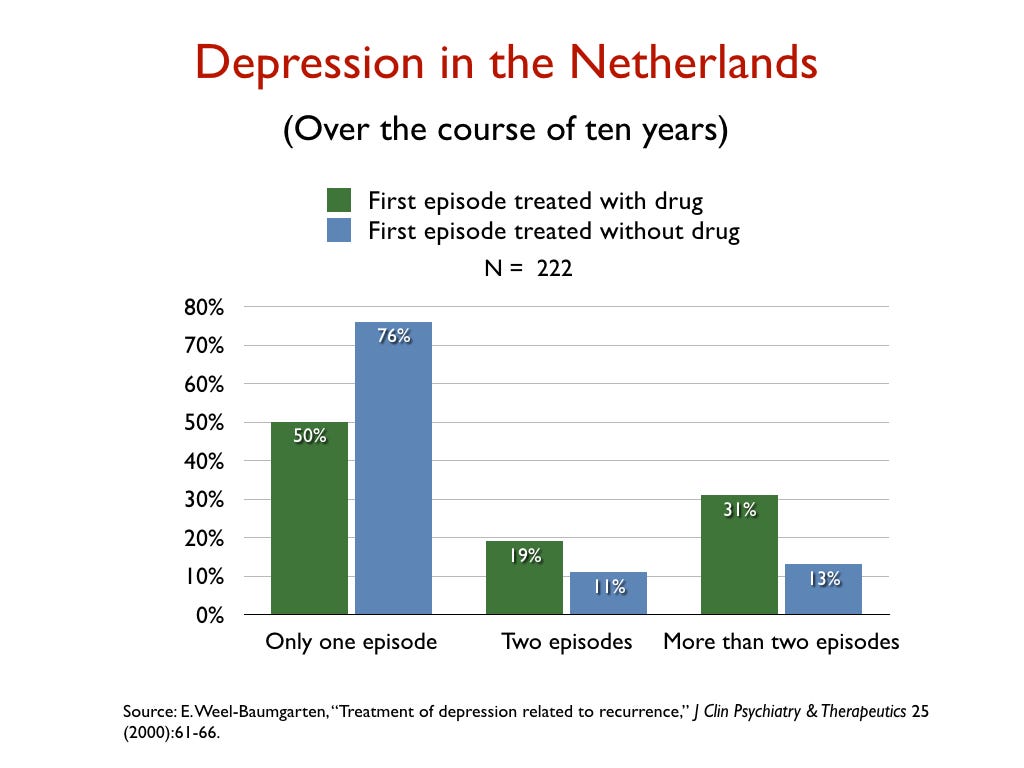
- In a retrospective study of the 10-year outcomes of 222 people who had suffered a first episode of depression, Dutch researchers reported that 76% of those not treated with an antidepressant recovered and never relapsed, versus 50% of those initially prescribed an antidepressant.

- In a Canadian study that charted outcomes for 9,508 depressed patients for five years, those taking antidepressants were depressed on average 19 weeks per year, versus 11 weeks for those not taking antidepressants.


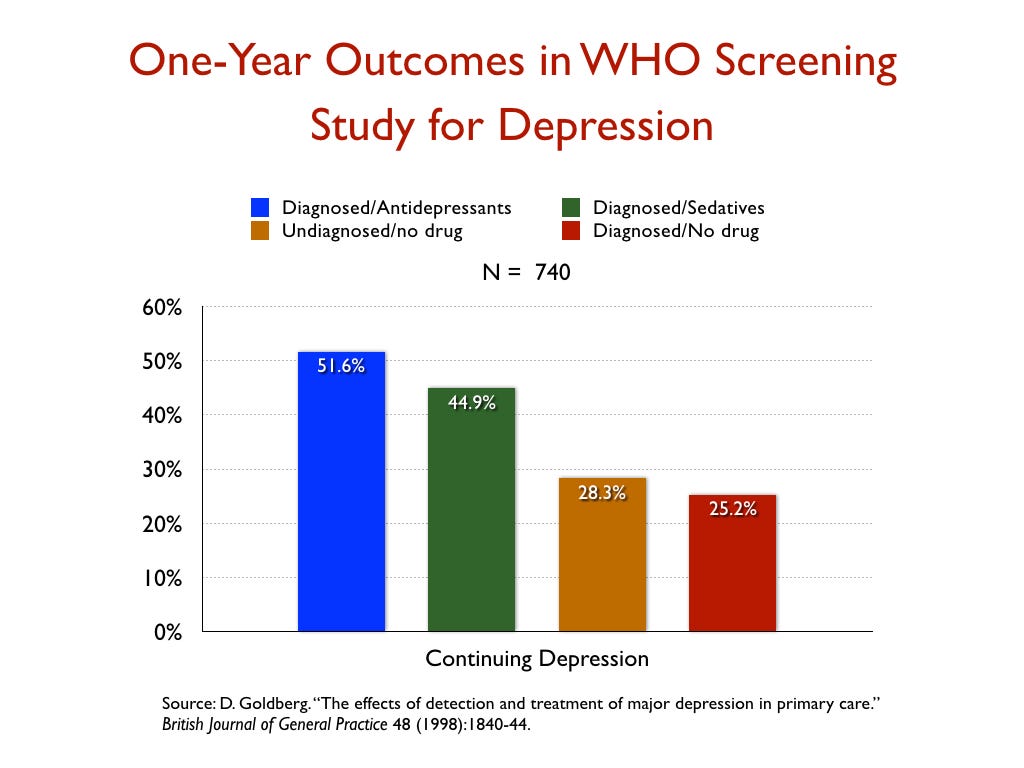
- In a World Health Organization study designed to assess the merits of screening for depression, which was conducted in 15 cities around the world, the patients who were diagnosed by their GPs and treated with an antidepressant were twice as likely to be depressed at the end of one year as those who weren’t diagnosed and treated, even though their baseline depression scores were nearly the same.

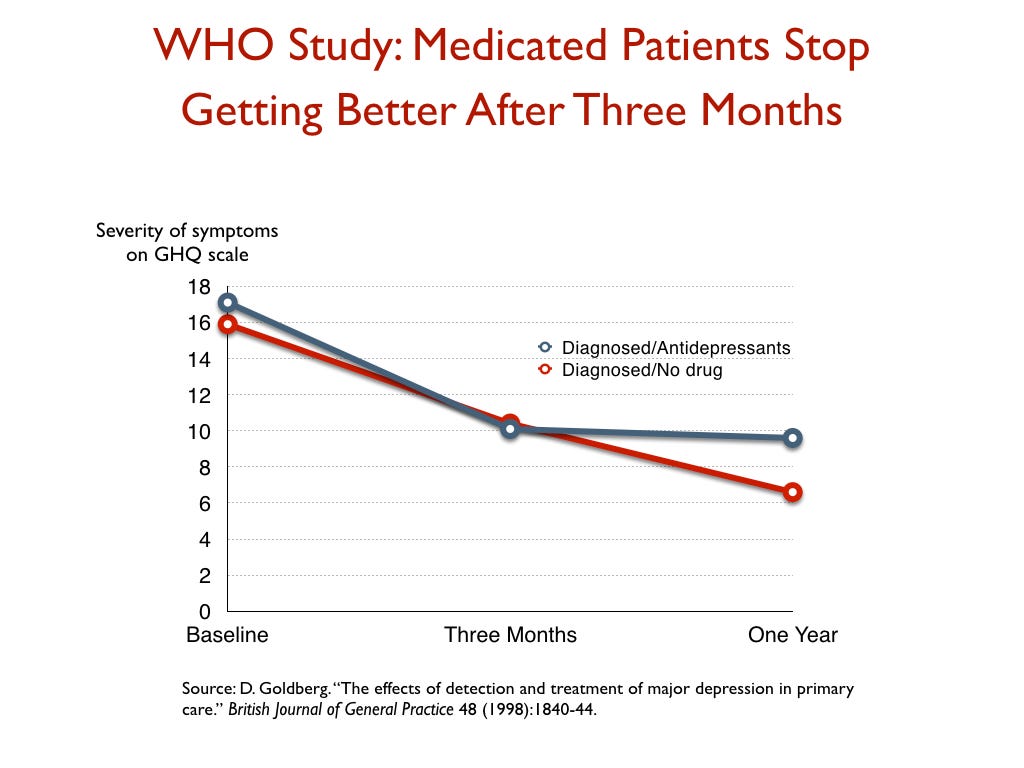
This WHO study also provided some insight into the effectiveness of antidepressants — or their lack of effectiveness — over time. At the end of three months, the patients treated with medications had improved slightly more than the unmedicated group, but after that time they stopped getting better, while the unmedicated group continued to improve throughout the year.

Disability studies
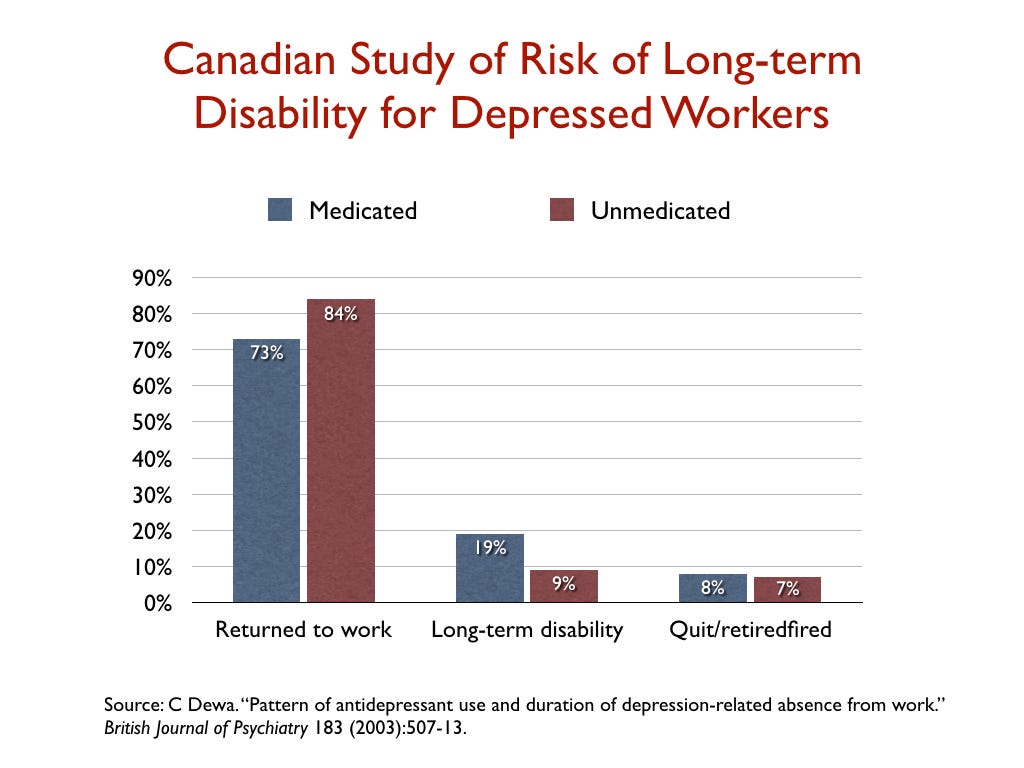
While most studies of depression focus on reduction of symptoms, a few researchers have looked at whether antidepressant use affects disability rates. In a study of 1,281 people who went on short-term disability in Canada due to depression, 19% of those who took an antidepressant failed to return to work and went on long-term disability, compared to 9% of those who didn’t fill a prescription.

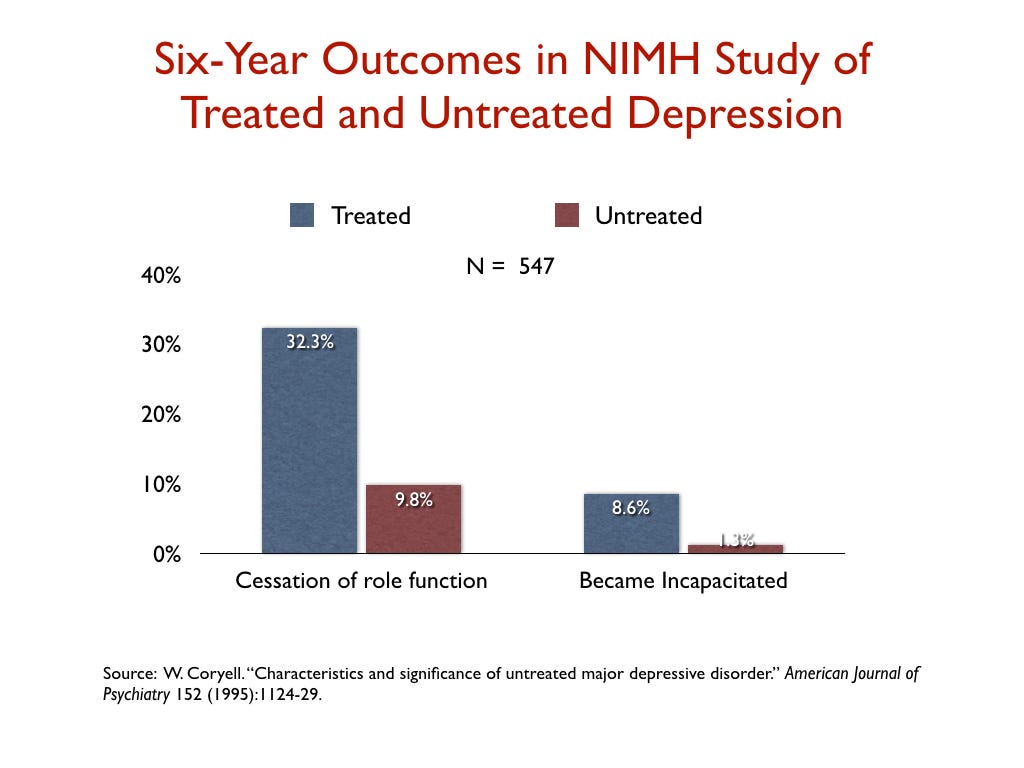
In a similar vein, an NIMH-funded study assessed the six-year “naturalistic” outcomes of 547 people who suffered a bout of depression, and found that those who were treated for the illness were three times more likely than the untreated group to suffer a “cessation” of their principal social role, and nearly seven times more likely to become incapacitated.

Summing up the people’s evidence
When psychiatry states that “antidepressants work,” the profession is telling of efficacy findings that emerge from RCTs, which are conducted in a small subset of real-world patients, and are fraught with design problems that favor the drug. Even so, the effect size favoring antidepressants is small, with an NNT of eight based on symptom scores.
In real-world populations, response and remission rates are lower, and they are particularly poor at the end of one year. Medication appears to provide few people with a sustained benefit, and there is substantial evidence that natural recovery rates are much higher. Medication also increases the risk that a person will become disabled by the disorder.
In addition, antidepressants may cause a wide range of adverse effects, which have not been listed here. This review of outcomes in real-world patient has focused on the “benefit” side of the question to assess whether antidepressants can be said to “work,” and even without subtracting the many risks from the benefits, the effectiveness studies provide reason for people to think twice before starting an antidepressant. The studies regularly tell of a treatment that increases the likelihood that patients will become chronically depressed.
Do antidepressants work for society?
The question of whether antidepressants “work” for society is different in kind than whether the drugs “work” for patients. The societal question requires a review of public health data: Does the treatment lead to a lessening of the societal burden from the disorder? Do antidepressants have this effect on depression?
Unfortunately, the public health data tell of a failed paradigm of care. The burden of depression in developed countries around the world has dramatically increased since Prozac arrived on the market in 1987. A 2015 study found that the economic burden from depression in the United States increased from $83 billion in 2000 to $210 billion in 2010.
In a similar vein, there has been a dramatic increase in the number of people on disability due to mood disorders in developed countries during the Prozac era, with this increase happening in lockstep with the increased prescribing of antidepressants. Given the disability studies conducted in the United States and Canada, this is precisely the public health outcome that one would expect.
Here are relevant disability statistics for five countries:

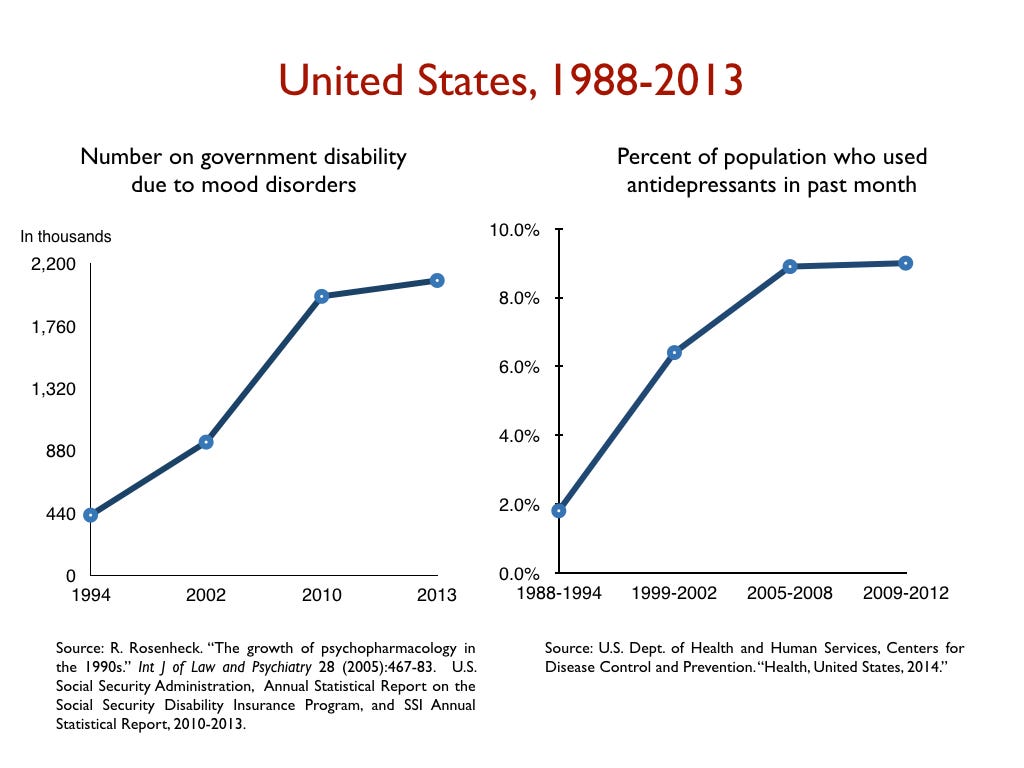



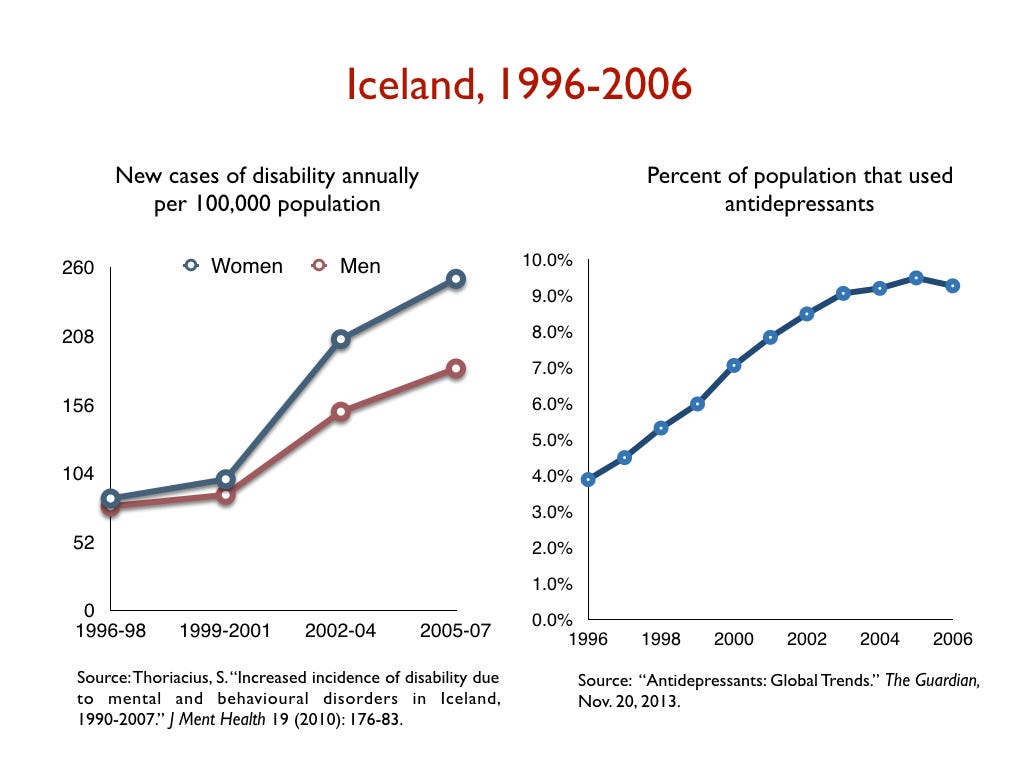




I think it is fair to conclude, based on this data, that antidepressants, as they are used now, can’t be said to “work” for society. Instead, they can be said to cause significant societal harm.
About Robert Whitaker
Robert Whitaker is a journalist and author of two books about the history of psychiatry, Mad in America and Anatomy of an Epidemic, and the co-author, with Lisa Cosgrove, of Psychiatry Under the Influence. He is the founder of madinamerica.com.
© 2018 Mad in America Foundation